DCS in Pharmaceutical: The Best Practitioner Guide to Distributed Control Systems in Pharma Plants
By Daniel Reed / June 23, 2026
I should be honest at the start of this article: my direct hands-on experience is in continuous oil and gas process control, not pharmaceutical batch manufacturing. I haven’t commissioned a DCS in a sterile bioreactor suite or signed off on a GAMP 5 validation package for a biotech facility.
What I have done is work across multiple DCS platforms (Honeywell Experion, Yokogawa CENTUM, Emerson DeltaV adjacent) and seen how regulatory framework, batch control discipline, and validation rigor reshape DCS engineering when the application moves from oil and gas to pharmaceuticals.
This article is my honest synthesis of what makes DCS in pharmaceutical fundamentally different from the continuous process control I do day-to-day. Some of it transfers directly — the DCS platforms are the same, the control loops still tune the same way, the operator interfaces follow the same ISA-101 principles.
But much of it is genuinely different — the regulatory framework reshapes everything, the batch control architecture follows ISA-88 in ways that continuous plants don’t need, and the validation discipline makes pharma DCS engineering its own specialty.
I’ll walk through the regulatory framework that defines pharmaceutical DCS work (FDA 21 CFR Part 11, EU Annex 11, GAMP 5), the ISA-88 batch control hierarchy that structures pharma automation, the major pharmaceutical process operations and their DCS challenges, the validation lifecycle that consumes more engineering effort than the configuration itself, and the vendor landscape where Emerson DeltaV and Siemens PCS 7 dominate in ways they don’t in oil and gas.
If you’ve read our DCS in Refining guide and DCS in LNG guide, this article closes the Applications cluster with the most regulatory-driven industry in process control.
TL;DR — Quick Answer: What Is DCS in Pharmaceutical?
DCS in pharmaceutical refers to the application of Distributed Control Systems to pharmaceutical manufacturing operations — both small molecule drug substance production and biologics manufacturing including bioreactors, downstream purification, formulation, and fill-finish. Unlike continuous process industries (refining, petrochemicals, LNG), pharmaceutical manufacturing is dominated by batch processing where each batch must be electronically documented for FDA and EMA regulatory compliance.
DCS in pharmaceutical operates under a unique regulatory framework: FDA 21 CFR Part 11 (electronic records and signatures), EU Annex 11 (computerized systems in GMP environments), and GAMP 5 (Good Automated Manufacturing Practice — the risk-based validation methodology). These regulations require formal validation of every computerized system, with documented evidence that the system performs as intended.
The structural framework for pharmaceutical batch automation is ISA-88 (the Batch Control standard), which defines the hierarchy of recipes, equipment modules, control modules, and procedural elements. Combined with ISA-95 for enterprise integration, ISA-88 enables the electronic batch records (EBR) that FDA-regulated manufacturers must maintain.
The major DCS platforms in pharmaceutical are Emerson DeltaV (strong ISA-88 batch and GAMP 5 compliance heritage), Siemens PCS 7 (particularly strong in European pharma), Honeywell Experion PKS, and Rockwell PlantPAx. Market share patterns differ significantly from oil and gas — DeltaV and PCS 7 are pharma leaders, while Yokogawa CENTUM is less common.
Key concepts for pharmaceutical DCS:
- Regulatory compliance is non-negotiable — every system must be validated to FDA/EMA standards
- Batch processing dominates — ISA-88 hierarchy structures all automation
- Electronic Batch Records (EBR) — every batch must be electronically documented
- GAMP 5 validation lifecycle — IQ, OQ, PQ documented for every system
- Audit-ready documentation — system documentation often exceeds the system itself
- Change control discipline — every modification requires formal change management
- Sterility and contamination control — physical process constraints unique to pharma
- Smaller scale than oil and gas — typical pharma DCS deployments are 3,000-15,000 I/O
What You Will Learn
This guide covers DCS in pharmaceutical at the depth working engineers genuinely need:
- Why pharmaceutical DCS is fundamentally different from continuous process DCS
- The regulatory framework: FDA 21 CFR Part 11, EU Annex 11, GAMP 5
- ISA-88 batch control hierarchy and how it structures pharmaceutical automation
- The major pharmaceutical process operations and their DCS challenges
- The validation lifecycle (User Requirements → DQ → IQ → OQ → PQ)
- Electronic batch records and integration with MES/ERP per ISA-95
- DCS platform considerations specific to pharmaceutical applications
- Common pharmaceutical DCS implementation mistakes documented in industry literature
Why DCS in Pharmaceutical Is Fundamentally Different
Pharmaceutical manufacturing has characteristics that set it apart from oil and gas and that reshape every aspect of DCS engineering.
DCS in pharmaceutical regulatory framework drives everything.
In oil and gas, DCS engineering follows good engineering practice and industry standards (ISA, IEC, API). Failure consequences are economic, safety, and environmental — significant, but bounded. In pharmaceutical, DCS engineering follows federal regulations enforced by agencies (FDA, EMA, MHRA) with the power to halt production, recall products, withdraw market authorization, and bring criminal charges. Patient safety is the ultimate consequence. Every aspect of DCS engineering changes in light of this.
The FDA’s 21 CFR Part 11 regulation specifies how electronic records and electronic signatures must be managed when used in FDA-regulated activities. Pharmaceutical DCS systems generate electronic records continuously — every alarm, every operator action, every setpoint change, every batch parameter — and all of it must be managed per Part 11 requirements.
DCS in pharmaceutical batch processing replaces continuous processing.
Oil and gas, refining, and LNG are continuous processes — feed flows in, products flow out, the plant runs for years between turnarounds. Pharmaceutical manufacturing is dominated by batch processing — discrete batches with defined start and end points, recipes that specify the production procedure, equipment that’s cleaned between batches, and quality testing of each batch before release.
This isn’t a minor difference. The entire control architecture changes. Where continuous processes need PID loops tuned for stable long-term operation, batch processes need sequential control following recipes through phases (heating, mixing, reacting, cooling, transferring). Where continuous processes log alarms and trend data, batch processes generate batch records that document every parameter for every batch.
ISA-88 structures the automation.
ISA-88 (the international standard for Batch Control) defines a hierarchical model: Process Cell → Unit → Equipment Module → Control Module. Recipes are structured to match: Site Recipe → Master Recipe → Control Recipe. Every batch is executed by combining recipes with physical equipment through this hierarchy.
In continuous process industries, ISA-88 exists but rarely dominates the automation architecture. In pharmaceutical, ISA-88 is the foundation that everything else builds on. DCS configuration follows the ISA-88 model. The MES (Manufacturing Execution System) speaks ISA-88. The batch records are organized per ISA-88 structure. Engineers working in pharma without strong ISA-88 understanding don’t last long.
DCS in pharmaceutical validation consumes more effort than configuration.
This is the difference that surprises engineers moving from oil and gas to pharmaceuticals. In oil and gas, DCS engineering effort is roughly 70% configuration and 30% testing/commissioning. In pharmaceutical, that ratio inverts. GAMP 5 validation lifecycle requirements mean that for every line of configuration, multiple validation documents must be created, reviewed, and approved. Installation Qualification (IQ), Operational Qualification (OQ), and Performance Qualification (PQ) protocols can consume more engineering hours than the configuration they validate.
Sterility and contamination control add physical constraints.
Pharmaceutical processes — especially biologics, sterile manufacturing, and aseptic operations — operate with sterility and contamination control requirements that don’t exist in oil and gas. Clean-in-place (CIP) and sterilize-in-place (SIP) cycles are major automation challenges. HVAC controls maintain cleanroom pressure cascades. Particulate monitoring integrates with the DCS. The physical process imposes constraints that reshape control system requirements.
Scale is generally smaller.
A large pharmaceutical manufacturing site might deploy 5,000-15,000 I/O on its DCS — small compared to a refinery (20,000-100,000+) or LNG plant (15,000-30,000). Multiple smaller production trains often replicate similar processes for different products, with each train independently validated. The engineering challenge is in the depth of validation and documentation rather than the breadth of I/O.
For broader DCS context, see our What Is a DCS cornerstone guide.
The Regulatory Framework — FDA Part 11, EU Annex 11, GAMP 5
Understanding DCS in pharmaceutical requires understanding the regulatory framework that shapes every engineering decision.
FDA 21 CFR Part 11 — Electronic Records and Electronic Signatures.
Issued by the FDA in 1997, 21 CFR Part 11 establishes the requirements for electronic records and electronic signatures used in FDA-regulated activities. For pharmaceutical DCS systems, Part 11 requires:
- Audit trails — every change to electronic records must be recorded with user, timestamp, and reason
- Electronic signatures — when used in place of handwritten signatures, must be uniquely attributable and non-repudiable
- System validation — computerized systems must be validated to ensure accuracy, reliability, and consistent intended performance
- Access controls — only authorized users may access systems; access levels must be appropriate to user role
- Data integrity — records must be protected from unauthorized modification; ALCOA principles (Attributable, Legible, Contemporaneous, Original, Accurate)
- Record retention — electronic records must be retained for periods specified by predicate rules (often years to decades)
Part 11 doesn’t tell engineers exactly how to implement compliance — it sets requirements, and implementation approaches are validated per GAMP 5.
EU Annex 11 — Computerised Systems.
Annex 11 to the EU GMP guidelines is the European equivalent of Part 11. The two regulations are conceptually similar but differ in some specifics. Multinational pharmaceutical manufacturers typically design systems to satisfy both — Part 11 for FDA-regulated production, Annex 11 for European production.
GAMP 5 — Good Automated Manufacturing Practice.
GAMP 5 isn’t a regulation — it’s a guidance document published by the International Society for Pharmaceutical Engineering (ISPE). But it has become the de facto industry methodology for validating computerized systems in pharmaceutical manufacturing. GAMP 5 provides:
- Risk-based validation methodology — validation effort scaled to system risk and complexity
- System categorization — Category 1 (infrastructure software), Category 3 (non-configured products), Category 4 (configured products), Category 5 (custom applications). DCS configuration typically falls in Category 4
- V-model lifecycle — User Requirements Specification → Functional Specification → Design Specification → Configuration → IQ → OQ → PQ → User Acceptance
- Supplier leveraging — Vendor documentation and testing can be leveraged rather than redundantly created by users
GAMP 5 reshapes how DCS engineering is documented. Where oil and gas DCS engineering produces functional design specs and control narratives, pharmaceutical DCS engineering produces a complete documented chain from user requirements through validation protocols.
The validation V-model.
The GAMP 5 V-model defines validation in two parallel tracks:
The design track (descending left side of the V):
- User Requirements Specification (URS) — what the user needs the system to do
- Functional Specification (FS) — what the system will do to meet requirements
- Design Specification (DS) — how the system will be configured to deliver the functionality
- Configuration and Coding — the actual DCS configuration
The validation track (ascending right side of the V):
- Installation Qualification (IQ) — verify the system is installed per specifications
- Operational Qualification (OQ) — verify the system operates per specifications
- Performance Qualification (PQ) — verify the system performs reliably in actual production use
Each validation step traces back to corresponding design specifications. The traceability matrix linking URS through PQ is itself a key deliverable.
ISA-88 Batch Control — The Foundation of Pharma DCS
ISA-88 (international equivalent IEC 61512) is the standard for batch control. While ISA-88 applies to any batch industry, pharmaceutical manufacturing is where it’s implemented with the deepest discipline.
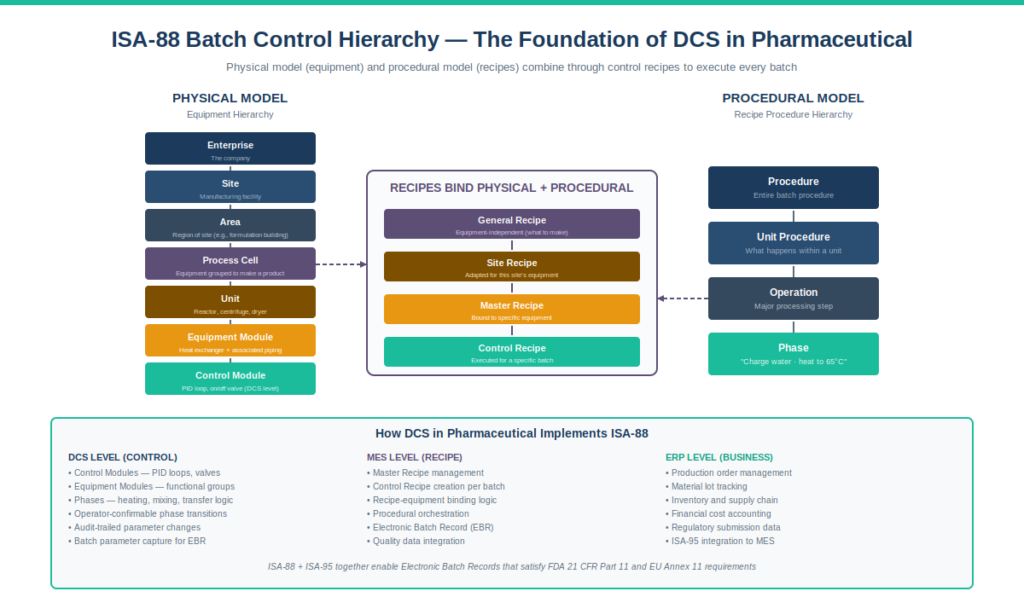
The ISA-88 physical model hierarchy.
ISA-88 defines a hierarchy of physical equipment in a batch facility:
- Enterprise — the company as a whole
- Site — a manufacturing facility
- Area — a region of a site (e.g., the formulation building)
- Process Cell — equipment grouped to make a batch product (e.g., the API production train)
- Unit — equipment that performs major processing operations (e.g., a reactor, a centrifuge, a dryer)
- Equipment Module — a functional group within a unit (e.g., the heat exchanger and its associated piping)
- Control Module — the lowest level of automation (e.g., a temperature control loop or an on-off valve)
DCS configuration follows this hierarchy. Control modules are configured at the lowest level. Equipment modules group control modules into functional units. Units are configured to execute phases (heating, mixing, transferring). Process cells coordinate units to execute batches.
The ISA-88 procedural model.
In parallel to the physical model, ISA-88 defines a procedural hierarchy:
- Procedure — the entire batch procedure
- Unit Procedure — what happens within a unit
- Operation — a major processing step within a unit procedure
- Phase — the lowest level of procedural element (e.g., charge water, heat to 65°C, add reagent A)
Phases are the building blocks of batch execution. A typical pharmaceutical batch procedure might consist of 50-200 phases executing in sequence and parallel. The DCS executes phases through configured logic; the MES coordinates the higher levels of the procedural hierarchy.
Recipes — the bridge between physical and procedural.
ISA-88 recipes combine procedural elements with the physical equipment they execute on:
- General Recipe — equipment-independent description (what to make)
- Site Recipe — adapted for a specific site’s equipment context
- Master Recipe — bound to specific equipment (which reactor, which sequence)
- Control Recipe — executed for a specific batch (which actual batch, when)
Each batch execution creates a Control Recipe from the Master Recipe, executes it against the physical equipment, and generates a Batch Record documenting what actually happened.
Why ISA-88 matters so much in pharmaceutical.
For pharmaceutical manufacturers, ISA-88 isn’t just an engineering convenience — it’s the structural framework that enables electronic batch records to satisfy FDA Part 11. The recipe structure, phase execution, and batch record generation all flow from ISA-88. Without rigorous ISA-88 implementation, the batch record can’t be reliably automated, which means manual batch records (slower, more error-prone, more expensive to validate). Pharmaceutical manufacturers consistently invest in deep ISA-88 implementation because the regulatory and operational payback is substantial.
For the broader enterprise integration framework that connects ISA-88 batch execution to MES and ERP, see our ISA-95 Enterprise Integration guide.
The Major Pharmaceutical Process Operations and Their DCS in Pharmaceutical Challenges
DCS in pharmaceutical manufacturing covers a wider range of process types than continuous industries. The major categories have distinct DCS in pharmaceutical challenges.
Small Molecule API Production.
Active Pharmaceutical Ingredient (API) production through chemical synthesis. Multi-step organic chemistry in stainless steel or glass-lined reactors, with intermediate isolation and purification. Similar in some ways to specialty chemicals but with stricter quality controls.
DCS challenges:
- Reactor temperature control — exothermic reactions require precise temperature management
- Multi-step batch sequencing — pharmaceutical syntheses can involve 15-30 batch steps
- Solvent recovery and handling — distillation columns for solvent recycling
- Crystallization control — particle size and crystal form affect drug bioavailability
- In-process control sampling — operator-prompted sampling at defined phases
Biologics and Bioreactor Operations.
Production of therapeutic proteins, vaccines, and cell therapies using living cells (mammalian, microbial, or insect). Fundamentally different from chemical synthesis — the production organism is a critical element of the process.
DCS challenges:
- Bioreactor environmental control — temperature, dissolved oxygen, pH, agitation, all tightly controlled to optimize cell growth
- Feed strategy automation — controlled glucose feeding (fed-batch) or perfusion control
- Sterility maintenance — every part of the bioreactor system must remain sterile throughout the production run
- Cell density monitoring — online and at-line measurements integrated with DCS
- Harvest sequencing — automated harvest at the optimal cell density and metabolic state
Downstream Processing (Purification).
Separating the target product from production cells, contaminants, and process residues. Heavy use of chromatography (affinity, ion exchange, size exclusion), filtration, and concentration operations.
DCS challenges:
- Chromatography column automation — column equilibration, loading, washing, elution, regeneration sequences
- UV detection integration — peak detection drives fraction collection decisions
- Filtration operations — tangential flow filtration with pressure and flow control
- Buffer preparation and management — multiple buffers required, each must be prepared and tracked
- Single-use systems integration — bag-based equipment with disposable sensors
Sterile and Aseptic Processing.
Production of sterile drug products (injectables, ophthalmics, sterile biologics). The most regulatorily stringent area of pharmaceutical manufacturing.
DCS challenges:
- Cleanroom HVAC control — pressure cascades, temperature, humidity, particulate counts
- CIP/SIP automation — clean-in-place and sterilize-in-place cycles fully automated
- Aseptic processing sequences — automated filling under sterile conditions
- Environmental monitoring integration — particulate counters, microbial monitors connected to DCS
- Gowning room access controls — interlocked airlock sequences
Solid Oral Dosage Manufacturing.
Production of tablets and capsules. Granulation, blending, compression, coating, packaging — a multi-step process with extensive equipment.
DCS challenges:
- Granulation control — wet granulation with spray rate and endpoint determination
- Fluid bed drying — temperature and humidity control with endpoint detection
- Tablet press automation — compression force, weight, hardness monitoring
- Coating operations — spray pattern, drying air control
- Process Analytical Technology (PAT) — NIR and Raman spectroscopy integrated with DCS for real-time quality
Fill-Finish Operations.
The final manufacturing step — filling drug product into vials, syringes, or other primary containers, sealing, and inspection.
DCS challenges:
- Filling accuracy — typically gravimetric or volumetric with tight precision requirements
- Stoppering and capping — sequenced operations with vision inspection
- Lyophilization control — freeze-drying with carefully controlled shelf temperature and chamber pressure profiles
- Visual inspection integration — automated inspection systems feeding accept/reject decisions
DCS in Pharmaceutical Platform Considerations
The DCS in pharmaceutical vendor landscape is significantly different from oil and gas. Market positioning reflects historical investment in batch control, ISA-88 compliance, and GAMP 5 validation support.
Emerson DeltaV — Strong Pharma Position.
DeltaV has invested heavily in pharmaceutical capabilities — DeltaV Batch is widely recognized for its ISA-88 implementation depth, and Emerson provides extensive GAMP 5 documentation packages that reduce validation burden. CHARMs I/O can simplify late-stage signal type changes (common in pharmaceutical projects where process definition continues evolving). DeltaV’s installed base in pharmaceuticals is substantial and continues growing.
For broader DeltaV context, see our Emerson DeltaV architecture guide.
Siemens PCS 7 — European Pharma Leader.
PCS 7 has particularly strong adoption in European pharmaceutical manufacturing, driven by Siemens’s deep presence in German and Swiss pharma manufacturing. SIMATIC BATCH for ISA-88 batch execution, integration with Siemens MES platforms, and CFC (Continuous Function Chart) programming all suit pharmaceutical engineering workflows.
Honeywell Experion PKS.
Experion has pharmaceutical deployments globally, particularly in larger pharma manufacturers with multi-industry presence. Experion Batch provides ISA-88 batch execution; Experion’s strength in safety system integration appeals to pharmaceutical operations with extensive sterile manufacturing and aseptic processing safety requirements.
For broader Experion context, see our Honeywell Experion PKS architecture guide.
Rockwell PlantPAx.
Rockwell’s process automation offering, built on the ControlLogix platform familiar to PLC engineers. PlantPAx has gained pharmaceutical market share, particularly in facilities that migrate from PLC-based systems toward DCS architecture while preserving Allen-Bradley familiarity.
Yokogawa CENTUM VP.
CENTUM has pharmaceutical deployments, particularly in Asian markets where Yokogawa has historical strength. Market share in pharmaceutical is smaller than in oil and gas, refining, or LNG.
For broader CENTUM context, see our Yokogawa CENTUM VP architecture guide.
ABB 800xA.
Has pharmaceutical deployments but smaller market share than DeltaV or PCS 7 in this industry specifically.
DCS in Pharmaceutical Validation Lifecycle — Where Most Engineering Effort Goes
The validation lifecycle is what makes DCS in pharmaceutical engineering uniquely demanding. Understanding it is essential to understanding why pharmaceutical projects take longer and cost more than equivalent oil and gas projects.
User Requirements Specification (URS).
The URS describes what the user needs the system to do — written in business and operational terms, not technical implementation. The URS is the foundational document; everything else traces back to it.
Typical URS contents:
- Process functional requirements (what unit operations the system must control)
- Operational requirements (operator interface, alarm handling, batch execution)
- Regulatory requirements (Part 11 compliance, audit trail requirements)
- Performance requirements (cycle times, throughput, accuracy)
- Integration requirements (MES, ERP, laboratory systems)
- Data integrity requirements
Functional Specification (FS).
The FS translates user requirements into functional design — what the system will do to meet each URS requirement. The FS is typically written by the engineering team and reviewed against the URS.
Design Specification (DS).
The DS describes how the system will be configured to deliver the FS functionality. For DCS in pharmaceutical, the DS covers function block design, batch recipe structure, HMI graphics design, alarm philosophy, and integration interfaces.
Configuration.
The actual DCS configuration work — building function blocks, configuring batch recipes, designing HMI graphics. In pharmaceutical, configuration follows standards even more strictly than in oil and gas, because every configuration decision must be traceable to design specifications.
Installation Qualification (IQ).
IQ verifies that the system has been installed per the design specifications. Documentation includes hardware serial numbers, software version numbers, network configuration verification, environmental conditions, and physical installation verification. IQ is typically conducted at the FAT (Factory Acceptance Test) and again at SAT (Site Acceptance Test) after installation at site.
Operational Qualification (OQ).
OQ verifies that the system operates per the functional specifications. Test protocols exercise every function the system is expected to perform. For DCS, OQ includes verification of every configured function block, every batch phase, every HMI graphic, every alarm, every report. OQ documentation is extensive.
Performance Qualification (PQ).
PQ verifies that the system performs reliably in actual production use. PQ typically requires multiple successful execution of representative processes under actual operating conditions. For pharmaceutical DCS, this means executing multiple complete batches with all process variations and verifying that batch records, quality data, and process performance all meet specifications.
Traceability Matrix.
The traceability matrix links every URS requirement through FS, DS, configuration, IQ test, OQ test, and PQ test. This matrix is itself a regulatory deliverable. It demonstrates that every requirement was implemented, configured, and tested. Maintaining traceability through change control over the system’s lifecycle is one of the ongoing engineering responsibilities.
Change Control.
Once a system is validated and in production, every change requires formal change control — change request, impact assessment, design update, configuration change, requalification, and approval. This discipline is what enables pharmaceutical manufacturers to maintain validated state over decades of operation while still allowing necessary changes.
Electronic Batch Records and ISA-95 Integration
Electronic Batch Records are central to modern DCS in pharmaceutical operations. They are central to modern pharmaceutical manufacturing. They replace paper batch records with electronic equivalents that provide better data integrity, faster batch release, and stronger regulatory submissions.
What an EBR contains.
A typical pharmaceutical batch record documents:
- Batch identification (product, batch number, manufacturing date)
- Equipment used (specific reactors, equipment serial numbers)
- Materials used (raw material lots, quantities, expiry dates)
- Process parameters (every setpoint and measured value at every phase)
- Operator actions (every operator-initiated action with operator identification and timestamp)
- Alarms and deviations (every alarm raised, every deviation from normal range)
- In-process control results (sampling results, online measurements)
- Quality test results (release testing, stability testing)
- Approvals (signed by authorized personnel for batch release)
How DCS supports EBR.
The DCS generates most of the data that flows into EBR — process parameters, alarms, operator actions. The MES typically owns the EBR application and pulls data from the DCS through standardized interfaces. The integration is governed by ISA-95, which defines how manufacturing systems exchange data with enterprise systems.
ISA-88 + ISA-95 working together.
For pharmaceutical batch operations, ISA-88 (batch control) and ISA-95 (enterprise integration) work together. ISA-88 defines how recipes and batches are structured at the control layer; ISA-95 defines how batch information flows up to MES, ERP, and quality systems. The technical report ISA-95.00.05 specifically addresses how the two standards combine, and pharmaceutical implementations rely on this combination extensively.
Data integrity throughout the chain.
FDA Part 11 data integrity requirements apply across the entire chain — from the DCS controller through MES through ERP. The DCS generates audit-trailed data with timestamps and user identification. The MES preserves data integrity as it processes the data into EBR. The ERP integrates batch data into enterprise reporting. Any break in data integrity at any layer creates a Part 11 compliance gap.
Common DCS in Pharmaceutical Mistakes
Based on industry documentation, published case studies, and conversations with engineers who have moved between oil and gas and DCS in pharmaceutical work, here are recurring mistakes:
Underestimating validation effort. Engineers moving to pharmaceutical from oil and gas consistently underestimate the validation effort. URS, FS, DS, configuration, IQ, OQ, PQ, traceability matrix — each deliverable consumes significant engineering hours. Industry experience suggests budgeting 2-3× the configuration effort for validation documentation alone.
Insufficient ISA-88 implementation discipline. ISA-88 isn’t optional in pharmaceutical batch — it’s the structural foundation. Implementations that compromise ISA-88 discipline (mixing procedural and equipment hierarchy, using non-standard recipe structures, skipping the phase abstraction layer) create batch execution and validation problems that compound over years.
Treating DCS in pharmaceutical Part 11 compliance as IT problem only. FDA Part 11 compliance affects the DCS configuration itself — audit trails on every change, electronic signatures on critical operations, access controls aligned to user roles. Treating Part 11 as the IT department’s problem rather than embedded in DCS engineering creates compliance gaps that emerge during FDA inspections.
Skipping HMI rationalization for DCS in pharmaceutical batch operations. Batch operators need different HMI design than continuous process operators. Phase-aware graphics, recipe progress indicators, manual operation guidance — pharmaceutical HMI design has specific requirements per ISA-101 that differ from oil and gas implementations.
Inadequate alarm rationalization. Pharmaceutical batch processes generate many alarms during phase transitions — startup, hold, transfer, end-of-batch. Without ISA-18.2 rationalization, batch operators face alarm floods that obscure genuinely important conditions.
Underspecifying environmental monitoring integration. Cleanroom HVAC, particulate counts, environmental conditions — these must integrate with DCS for sterile manufacturing. Underspecified integration creates regulatory exposure when environmental conditions need to be correlated with batch parameters.
Treating CIP/SIP as secondary. Clean-in-place and sterilize-in-place cycles are major automation challenges. Pharmaceutical CIP/SIP must achieve documented cleaning and sterilization with full validation. Treating these cycles as utility operations rather than core batch operations creates engineering gaps.
Inadequate change management discipline. Validated state must be maintained over decades. Casual configuration changes, undocumented modifications, or shortcuts in change control destroy the validated state and create regulatory liability. Change management discipline must match the regulatory framework.
Insufficient FAT for batch execution. Factory Acceptance Testing in pharmaceutical must verify complete batch execution under realistic conditions. Skipping comprehensive batch execution testing during FAT defers problems to site commissioning, where they’re more expensive to resolve.
Ignoring Process Analytical Technology (PAT) integration. Modern pharmaceutical manufacturing increasingly integrates PAT — NIR spectroscopy, Raman spectroscopy, mass spectrometry — for real-time quality measurement. DCS architectures that don’t accommodate PAT integration create technical debt as PAT adoption expands.
Underestimating supplier audit requirements. Pharmaceutical manufacturers audit their DCS vendors per GAMP 5 supplier leveraging principles. Vendor documentation, vendor testing, and vendor support practices all come under audit scrutiny. Vendor selection must consider audit readiness, not just technical capability.
Frequently Asked Questions
What is DCS in pharmaceutical?
DCS in pharmaceutical refers to the application of Distributed Control Systems to pharmaceutical manufacturing operations — including small molecule API production, biologics manufacturing (bioreactors, downstream purification), sterile and aseptic processing, solid oral dosage manufacturing, and fill-finish operations. Pharmaceutical DCS operates under FDA 21 CFR Part 11, EU Annex 11, and GAMP 5 frameworks, with ISA-88 batch control as the structural foundation.
Which DCS platforms are most common in pharmaceutical?
Emerson DeltaV and Siemens PCS 7 are the most common platforms in pharmaceutical manufacturing. DeltaV is widely recognized for its ISA-88 batch implementation depth and GAMP 5 documentation; PCS 7 has particularly strong adoption in European pharmaceutical manufacturing. Honeywell Experion PKS, Rockwell PlantPAx, Yokogawa CENTUM VP, and ABB 800xA all have pharmaceutical deployments but smaller market share specifically in pharma.
What is GAMP 5?
GAMP 5 (Good Automated Manufacturing Practice, Version 5) is the industry-standard methodology for validating computerized systems in pharmaceutical manufacturing. Published by ISPE (International Society for Pharmaceutical Engineering), GAMP 5 provides risk-based validation guidance through the V-model lifecycle (User Requirements → Functional Spec → Design Spec → Configuration → IQ → OQ → PQ). It’s the de facto methodology for satisfying FDA Part 11 and EU Annex 11 validation requirements.
What is FDA 21 CFR Part 11?
FDA 21 CFR Part 11 is the FDA regulation governing electronic records and electronic signatures in FDA-regulated activities including pharmaceutical manufacturing. It requires system validation, audit trails, electronic signatures, access controls, data integrity, and record retention. Part 11 compliance is mandatory for FDA-regulated pharmaceutical operations using electronic records.
What is ISA-88?
ISA-88 (international equivalent IEC 61512) is the international standard for Batch Control, defining hierarchical models for batch processes — Physical Model (Process Cell → Unit → Equipment Module → Control Module) and Procedural Model (Procedure → Unit Procedure → Operation → Phase). ISA-88 is the structural foundation for pharmaceutical batch automation, enabling electronic batch records and modular recipe management.
How is pharmaceutical DCS different from oil and gas DCS?
Pharmaceutical DCS differs in several fundamental ways: (1) batch processing dominates instead of continuous processing, (2) regulatory framework (FDA Part 11, EU Annex 11, GAMP 5) shapes every engineering decision, (3) ISA-88 batch control is the structural foundation, (4) validation lifecycle consumes more engineering effort than configuration, (5) scale is generally smaller (3,000-15,000 I/O vs 20,000-100,000 in refining), and (6) vendor market share differs significantly (DeltaV and PCS 7 lead in pharma; CENTUM, Experion lead in oil and gas).
What is an Electronic Batch Record?
An Electronic Batch Record (EBR) is the electronic equivalent of a paper batch record — a complete documented record of how a specific batch was manufactured. EBR includes batch identification, equipment used, materials and quantities, process parameters at every phase, operator actions, alarms and deviations, in-process and quality testing, and authorized approvals. EBR is typically managed by MES (Manufacturing Execution System) integrated with DCS per ISA-95.
What is the V-model in GAMP 5?
The GAMP 5 V-model is the validation lifecycle that links design specifications (descending track) to validation testing (ascending track). The descending track moves from User Requirements Specification → Functional Specification → Design Specification → Configuration. The ascending track moves from Installation Qualification (IQ) → Operational Qualification (OQ) → Performance Qualification (PQ). Each validation step traces back to corresponding design specifications through a traceability matrix.
How much does pharmaceutical DCS validation cost?
Validation documentation typically consumes 2-3× the engineering effort of configuration itself. For a pharmaceutical DCS project of moderate scale (5,000-10,000 I/O), validation documentation including URS, FS, DS, IQ, OQ, PQ, and traceability matrix can represent 50-70% of total project engineering hours. The cost is driven by documentation depth, formal review cycles, and qualified validator effort.
Does pharmaceutical DCS use SIS?
Yes, pharmaceutical operations use Safety Instrumented Systems where the process hazards justify SIL-rated protection. Examples include sterile manufacturing where contamination could harm patients, high-pressure reactor systems, hazardous solvent handling, and aseptic processing isolators. The SIS in pharmaceutical typically follows the same IEC 61508/61511 framework as other industries, with the addition of GMP and Part 11 considerations for the integrated documentation. For broader SIS context, see our Safety Instrumented System guide.
Conclusion
DCS in pharmaceutical represents the most regulatorily-driven application of distributed control systems in process industries. The combination of FDA 21 CFR Part 11, EU Annex 11, GAMP 5 validation methodology, ISA-88 batch control discipline, and electronic batch records creates engineering requirements that fundamentally reshape DCS practice compared to continuous process industries.
The most important practical truths about DCS in pharmaceutical:
- DCS in pharmaceutical regulatory framework drives every engineering decision — FDA Part 11, EU Annex 11, and GAMP 5 are not optional
- DCS in pharmaceutical batch processing dominates — ISA-88 is the structural foundation that everything builds on
- Validation lifecycle consumes more engineering effort than configuration itself
- Electronic batch records require integration with MES per ISA-95
- Change control discipline must be maintained over decades of operation
- DeltaV and PCS 7 lead the DCS in pharmaceutical market — vendor selection patterns differ from oil and gas
- Scale is smaller than oil and gas, but documentation depth is dramatically greater
If you’re an engineer moving from continuous process industries into DCS in pharmaceutical work, expect to spend significant time learning the regulatory framework before you become productive. The DCS platform skills transfer; the validation discipline and regulatory mindset are genuinely new. The engineers who succeed in this transition develop deep respect for the documentation requirements rather than treating them as bureaucratic overhead.
If you’re approaching DCS in pharmaceutical project planning, resist the temptation to estimate based on oil and gas norms. Validation effort, change control discipline, and supplier audit requirements all extend project timelines significantly. Engage compliance and quality teams early — they’re not project obstacles, they’re co-engineers whose discipline is essential to a successful validated outcome.
I’ll close with the honest acknowledgment I started with: my direct experience is in continuous oil and gas process control, not pharmaceutical batch manufacturing. The framework above synthesizes what’s documented in industry standards (FDA, EMA, ISPE, ISA), what’s published in vendor literature, and what’s discussed by engineers who have worked across both domains.
For engineers actually working in pharmaceutical DCS, this article should serve as a structural overview — the deep details of GAMP 5 implementation, specific validation protocols, and platform-specific batch configuration come from working in the discipline itself.
For broader DCS context, see our What Is a DCS cornerstone guide. For platform-specific implementation, see our Emerson DeltaV architecture guide (the leading pharmaceutical DCS platform), Honeywell Experion PKS architecture guide, and Yokogawa CENTUM VP architecture guide.
For control theory underlying pharmaceutical critical loops, see our PID Tuning Methods guide.
For the foundational standards covered throughout this guide, see our ISA-101 HMI Design guide, ISA-18.2 Alarm Management guide, and ISA-95 Enterprise Integration guide.
For the sibling Applications articles covering continuous process domains, see our DCS in Refining guide and DCS in LNG guide.
About the Author
Daniel Reed is an Instrument and Controls Engineer with 14+ years of oil and gas EPC experience across onshore and offshore projects in Asia and Africa. He currently works as a client-side I&C completion engineer on a large oil and gas mega-project in Asia, where he has been involved with Honeywell Experion PKS and Safety Manager since 2018.
His earlier work covered Yokogawa CENTUM and Triconex SIS on an offshore brownfield in Africa (2015-2018), and Yokogawa CENTUM and ProSafe-RS on a gas-to-liquids facility in Africa. His focus is engineering deliverable review, control and safety system commissioning, HAZOP/SIL/SIF participation, FAT/SAT execution, and vendor coordination across Honeywell, Yokogawa, Triconex, Allen-Bradley, and Siemens platforms.
His direct hands-on experience is in continuous oil and gas process control rather than pharmaceutical batch manufacturing. This article synthesizes documented industry standards, published vendor literature, and cross-domain discussions with engineers who work in pharmaceutical DCS, rather than first-person pharmaceutical batch experience.